
We all know regular exercise is essential for good health. It can improve the fitness of your heart and lungs, sleep quality, energy levels and mental wellbeing. And it can reduce your risk of developing conditions such as diabetes.
Exercise is also vital for the health of your bones.
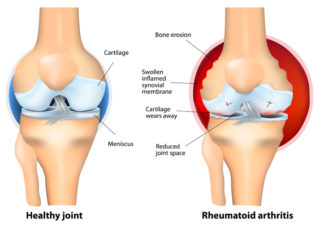
Like muscle, bone is living tissue that responds to exercise by becoming stronger. People who exercise regularly have stronger bones and higher bone density than those who don’t. This reduces the risk of developing osteoporosis.
Exercise also increases your balance, coordination and flexibility, which improves your ability to prevent trips and falls. DYK, falls are Australia’s largest contributor to injuries that require a stay in hospital and are a leading cause of injury deaths? More than half of the hospitalisations were due to broken bones (fractures).(1)
Bones need exercise.
To understand why exercise is important for bone health, it helps to know how bones work.
Throughout your life, your bones are constantly changing. This is called ‘remodelling’. Bone cells called osteoblasts build new bone, while other bone cells (osteoclasts) break down and remove old bone. This process is controlled by hormones such as calcitonin, parathyroid hormone, oestrogen (in women), testosterone (in men), and vitamin D.
From birth to about 25, you build more bone than you lose. Your bones are not only getting bigger as you grow, but they’re also developing their density. This determines how strong they are.
From about 25 to 50, your bones break down and rebuild at about the same rate. They’re in a state of balance. This is when you’ve achieved your ‘peak bone mass’. Your bones are at their strongest.
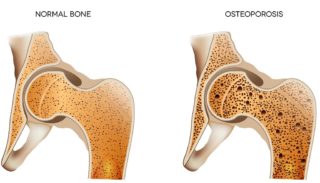
After about 50, you break down more bone than you rebuild. While this means everyone will experience some bone loss as they age, it doesn’t mean everyone will develop osteoporosis.
Women commonly experience a period of rapid bone loss after menopause. This is due to a drop in oestrogen levels. It’s estimated that the average woman loses up to 10% of her bone mass in the first five years after menopause.(2)
For good bone health, exercise is vital for everyone – from the very young to the very old.
A combination of different exercises is best for bone health.
Different exercises challenge and strengthen your bones and muscles in different ways, so you should include the following in your exercise plan:
Weight-bearing exercises or activities where your body carries its own weight. These exercises put stress on your bones, making them stronger and denser. It also strengthens the muscles around your bones, providing support and reducing the risk of fractures. Weight-bearing exercises include brisk walking, climbing stairs, tennis, and netball.
High-impact exercises such as jogging, running, jumping, and skipping rope. They’re also weight-bearing exercises, but they place greater stress on the bones of the spine and legs as your feet hit the ground. This can provide more bone-strengthening benefits; however, these exercises aren’t suitable for everyone.
Resistance training, also known as strength training, uses resistance or weights to strengthen your muscles by working them harder than you do in everyday life. The strong muscle contractions required to move a heavy weight place stress on the bone where the muscle attaches. When bone feels this strain repeatedly, it responds by becoming stronger. Resistance training uses equipment like free weights (e.g. dumbbells), gym machines, elastic resistance bands or your body weight (e.g. push-ups, squats).
Balance and flexibility exercises such as tai chi and yoga improve balance and mobility and can reduce your risk of falling. This is important for preventing fractures.
Before beginning an exercise program, speak with your health professional. Not all types of exercise are suitable for everyone. This is especially important if you have other health conditions, including osteoporosis. A physiotherapist or exercise physiologist can assist you with a safe exercise program that targets your specific needs and reduces your risk of injury.
Exercise must be regular and ongoing.
You need to exercise regularly to have a significant benefit, so you should choose activities you enjoy. This will make it easier to exercise consistently.
Australian physical activity and exercise guidelines recommend that all adults be active most days, preferably every day, for 30 minutes or more. This includes at least two sessions of strength training every week. However, when you’re just beginning, this can seem daunting.
That’s why it’s good to know you don’t have to do all your exercise in one session. For example, a 30-minute brisk walk can be broken up across your day into shorter, more achievable sessions, such as three 10-minute or six 5-minute walks.
You can do other things to make exercise a regular, ongoing activity.
Exercise with a group or a partner. This can improve your motivation to exercise and provides an opportunity for socialising with others.
Exercise SMART and set goals. A clear goal can motivate you to stay on track with your exercise program. But they must be realistic and specific to your abilities, needs, and health issuehttps://msk.org.au/goals/s. So, ensure your goal is SMART – Specific, Measurable, Achievable, Realistic and has a Timeframe.
For example, a good SMART goal for resistance training for stronger bones and muscles could be: “I will perform resistance exercises, such as lifting weights or using resistance bands, for 30 minutes, twice a week, for the next three months.”
This goal is Specific (focuses on resistance training), Measurable (30 minutes, twice a week), Achievable (realistic for most people), Relevant (aimed at improving bone and muscle strength), and has a Timeframe (three months).
Constantly evaluate your goals, adjust them as needed and reward yourself for your successes.
Add variety. Vary where you exercise and the type of exercise you do. Include recreational activities such as bushwalking or dancing. This will help keep your mind fresh and your motivation high. Find activities that are enjoyable to you so that you’ll be motivated to continue doing them.
Exercise within your capabilities. Often, people drop out of exercise programs because they exercise at a level beyond their current capabilities. Ensuring your exercise program suits your current abilities will decrease your risk of injury and increase your enjoyment and motivation to continue your exercise program.
Challenge yourself. Increase the intensity of your exercise as your fitness improves. It’ll make your exercise more interesting and also has greater health benefits.
Stop if you have pain. Don’t continue exercising if you experience pain or severe discomfort. Talk with your fitness professional for advice to ensure you’re not doing an exercise incorrectly.
Bone health doesn’t happen in a vacuum.
As well as exercise, you need to also to eat a nutritious diet with calcium-rich foods, get sufficient sun exposure for vitamin D, take medicines or supplements as prescribed by your doctor, quit smoking, and moderate your use of alcohol, caffeine, and salt intake, as they can impact bone density.
Contact our free national Help Line
Call our nurses if you have questions about managing your pain, musculoskeletal condition, treatment options, mental health issues, telehealth, or accessing services. They’re available weekdays between 9am-5pm on 1800 263 265; email (helpline@msk.org.au) or via Messenger.
More to explore
- Exercise
International Osteoporosis Foundation - Exercise
Osteoporosis Canada - Exercise & bone health
Healthy Bones Australia - Exercise and bone health
American Academy of Orthopaedic Surgeons - Exercise for bones
Royal Osteoporosis Society - Exercise for your bone health
NIH Osteoporosis and Related Bone Diseases, National Resource Center - Healthy living & bone health
Jean Hailes - Osteoporosis and exercise
Better Health Channel
References
(1) Falls. Australian Institute of Health and Welfare.
(2) Osteoporosis, Australasian Menopause Society